Clinical
Prescribing adds for accommodation lag
In this article:
Essential reading to preface the below are my notes on how to measure near lag of accommodation and how to measure accommodative facility. You can also watch how to measure accommodative lag on our Youtube channel.
You'll have already read how assessing accommodative function at near is a vital component of understanding the myopia profile of your patient. Myopic progression in children and adults can be influenced by binocular vision function. There is a reported association between higher levels of esophoria and accommodative lag at near in myopic children and young adults as compared to emmetropes.1-5 Myopic children and young adults also show insufficient accommodative responses to lens-induced blur,1, 6-8 greater variability in accommodative response9, reduced accommodative facility4, 8 and enhanced accommodative convergence (elevated AC/A ratios) when compared to age matched emmetropes.10-12 There is speculation in the literature regarding accommodative lag prior to onset of myopia - evidence shows higher accommodative lag in progressing myopes, regardless of their starting point of refraction as an emmetrope or myope,4 however other studies do not match this significance.13 Myopia development and progression is multifactorial, though, that it's important to assess all contributory factors - the myopia profile is designed to guide you through this clinical decision making and communication process.
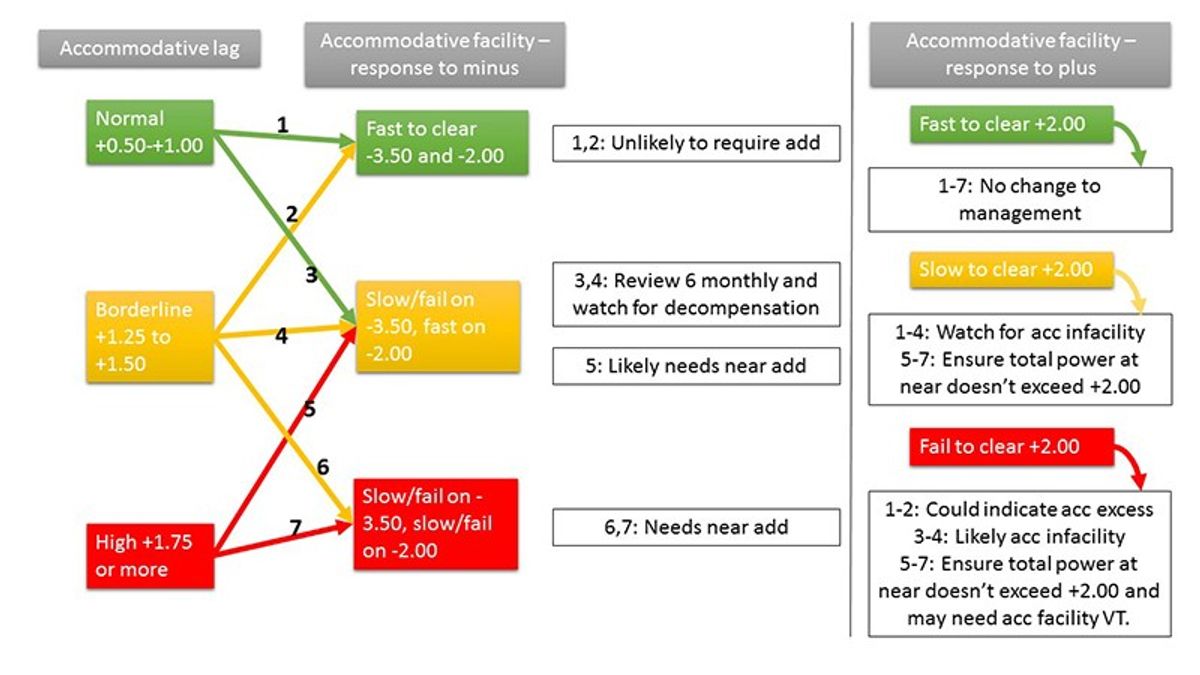
Prescribing adds for accommodative lag, when regarding the accommodative system in isolation, will generally depend on the magnitude of the lag, and the stamina to manage it. I describe this to my patients and their parents as the posture (lag) and petrol in the tank (facility/amplitude). Recall that a normal accommodative lag falls between +0.50 and +1.00 inclusive, with results higher than this indicating an increased risk for the myopia profile.4, 5, 11, 16, 17 We would also expect our young patient to be able to clear up to -3.50 at near point (a normal positive relative accommodation result) and +2.00 (a normal negative relative accommodation result) which measures part of the accommodative response in reference to demand. As described in my blog on how to measure accommodative facility, seeking qualitative observations on how your patient responds to both plus and minus over the course of several cycles enhances your clinical detail.
With these pieces of information, you can determine how well the 'posture' matches the 'petrol in the tank', and whether any support is needed. Look at the lag and the ability to clear minus first, and then look at the ability to clear plus to determine your prescribing choice. I'll explain with a flow chart:
Given that a normal lag result is +0.50, I would generally prescribe an add which is the accommodative lag result subtracting 0.50, so the resulting final lag is within the normal range. For example, a lag of +2.00 results in a +1.50 Add; a lag of +1.50 results in a +1.00 Add.
However, this formula may not work if:
- Your patient can't clear +2.00 at near and their distance refraction + ideal add is greater than +2.00 total - don't ask them to clear more in their specs than they've demonstrated during testing. Drop the add so you know they can see through it.
- The ideal add is too high for their working distance - for example, I'd rarely prescribe an add higher than +1.50 for high school aged children, to take into account computer working distances. You may be happy prescribing a higher add, though, in a progressive lens as compared to a bifocal or single vision near.
If your patient can't clear +2.00 at near, they may have accommodative excess / infacility as described above in the flowchart. In this case be careful of how much plus at near they will tolerate - you may need to prescribe accommodative facility vision training (VT), which is most easily achieved by reading through plus/minus flippers for 20 minutes per day, flipping every sentence to challenge the accommodative response to demand.
You may also want to prescribe more plus than the near lag (provided it will be tolerated, as indicated by their ability to clear +2.00) if you've got a significant esophoria at near and find the extra plus beneficial for its control - come back soon for more information on assessing fusional reserves at near, assessing near phoria and prescribing adds for near esophoria.
Try out your clinical thinking process with your patients using this flowchart, and please drop me a line in the comments below if you have any comments, questions or suggestions.
To delve more into my simplified two-system approach to BV diagnosis and management, you can watch this video entitled Binocular Vision - easier than you think. This one hour lecture includes cases; details easy use of prism correction for vergence disorders; changes to BV in contact lens wear; and why BV matters - for reading and learning in kids, clinical problem solving, and myopia management. You can also download my lecture notes here.
Want to learn more about binocular vision?
Check out my online course Binocular Vision Fundamentals, which starts with my two-system approach to BV assessment and diagnosis. Stepping through understanding of the accommodation and vergence systems, the course then covers clinical tests, diagnostic criteria, prescribing and management. Once this foundation is set, it moves onto clinical communication and the importance of BV in myopia management. Always with a laser sharp focus on the clinical applications.
Included are video examples of assessment techniques and chairside infographic summary downloads to reference in practice.
You can enroll on the first two modules for free, with the full course priced at US$140 if you decide to continue. Reduced course fees by 30% and 50% are available by application for practitioners residing in lower income countries - check out the course page for more information.
Meet the Authors:

About Kate Gifford
Dr Kate Gifford is an internationally renowned clinician-scientist optometrist and peer educator, and a Visiting Research Fellow at Queensland University of Technology, Brisbane, Australia. She holds a PhD in contact lens optics in myopia, four professional fellowships, over 100 peer reviewed and professional publications, and has presented almost 300 conference lectures around the world. Kate is the Chair of the Clinical Management Guidelines Committee of the International Myopia Institute. In 2016 Kate co-founded Myopia Profile with Dr Paul Gifford; the world-leading educational platform on childhood myopia management. After 13 years of clinical practice ownership, Kate now works full time on Myopia Profile.
References
- Gwiazda J, Bauer J, Thorn F, Held R. A dynamic relationship between myopia and blur-driven accommodation in school-aged children. Vision Res. 1995;35:1299-1304. (link)
- Nakatsuka C, Hasebe S, Nonaka F, Ohtsuki H. Accommodative lag under habitual seeing conditions: comparison between myopic and emmetropic children. Jap J Ophthalmol. 2005;49:189-194. (link)
- Drobe B, de Saint-André R. The pre-myopic syndrome. Ophthal Physiol Opt. 1995;15:375-378. (link)
- Allen PM, O'Leary DJ. Accommodation functions: Co-dependency and relationship to refractive error. Vision Res. 2006;46:491-505. (link)
- Price H, Allen PM, Radhakrishnan H, Calver R, Rae S, Theagarayan B, Sailoganathan A, O'Leary DJ. The Cambridge Anti-Myopia Study: Variables Associated with Myopia Progression. Optom Vis Sci. 2013;90:1274-1283. (link)
- Bullimore MA, Gilmartin B, Royston JM. Steady-state accommodation and ocular biometry in late-onset myopia. Documenta Ophthalmologica. Advances In Ophthalmology. 1992;80:143-155. (link)
- Abbott ML, Schmid KL, Strang NC. Differences in the accommodation stimulus response curves of adult myopes and emmetropes. Ophthal Physiol Opt. 1998;18:13-20. (link)
- Pandian A, Sankaridurg PR, Naduvilath T et al. Accommodative Facility in Eyes with and without Myopia. Invest Ophthalmol Vis Sci. 2006;47:4725-4731. (link)
- Harb E, Thorn F, Troilo D. Characteristics of accommodative behavior during sustained reading in emmetropes and myopes. Vision Res. 2006;46:2581-2592. (link)
- Gwiazda J, Grice K, Thorn F. Response AC/A ratios are elevated in myopic children. Ophthal Physiol Opt. 1999;19:173-179. (link)
- Gwiazda J, Thorn F, Held R. Accommodation, accommodative convergence, and response AC/A ratios before and at the onset of myopia in children. Optom Vis Sci. 2005;82:273-278. (link)
- Mutti DO, Jones LA, Moeschberger ML, Zadnik K. AC/A Ratio, Age, and Refractive Error in Children. Invest Ophthalmol Vis Sci. 2000;41:2469-2478. (link)
- Rosenfield M, Desai R, Portello JK. Do progressing myopes show reduced accommodative responses? Optom Vis Sci. 2002;79:268-273. (link)
- Zhu M, Feng H, Zhu J, Qu X. The impact of amplitude of accommodation on controlling the development of myopia in orthokeratology]. Chinese J Ophthalmol. 2014;50:14-19. (link)
- Evans BJW. Detecting binocular vision anomalies in primary eyecare practice. Pickwell's Binocular Vision Anomalies (Fifth Edition). Edinburgh: Butterworth-Heinemann; 2007:12-38. (link)
Enormous thanks to our visionary sponsors
Myopia Profile’s growth into a world leading platform has been made possible through the support of our visionary sponsors, who share our mission to improve children’s vision care worldwide. Click on their logos to learn about how these companies are innovating and developing resources with us to support you in managing your patients with myopia.