Clinical
The esophoric myope and contact lenses
In this article:
When it comes to contact lens corrections for young myopes, the impact of orthokeratology (OK) and multifocal soft contact lenses (MFSCL) on binocular vision is pertinent to visual comfort and understanding mechanisms of myopia progression and control.
Oliver's story
Oliver, age 10, was referred with a history of fast, recent myopia progression. His mother was R&L -7.00 and he was quickly catching up - his refractive history was reported as being R&L -2.75 at age 7; R -4.00 L -4.50 at age 8; R -4.75 L -5.25 at age 9 and now R -6.00 L -6.75 at age 10. Only a month after seeing his referring optometrist, his acuity with this latter correction was R 6/12 and L 6/19, with retinoscopy over his spectacles revealing an extra 1D of myopia in each eye. Cycloplegic retinoscopy revealed R -6.50 and L -5.75 which didn't appear to align with his presenting acuity in this newest prescription.
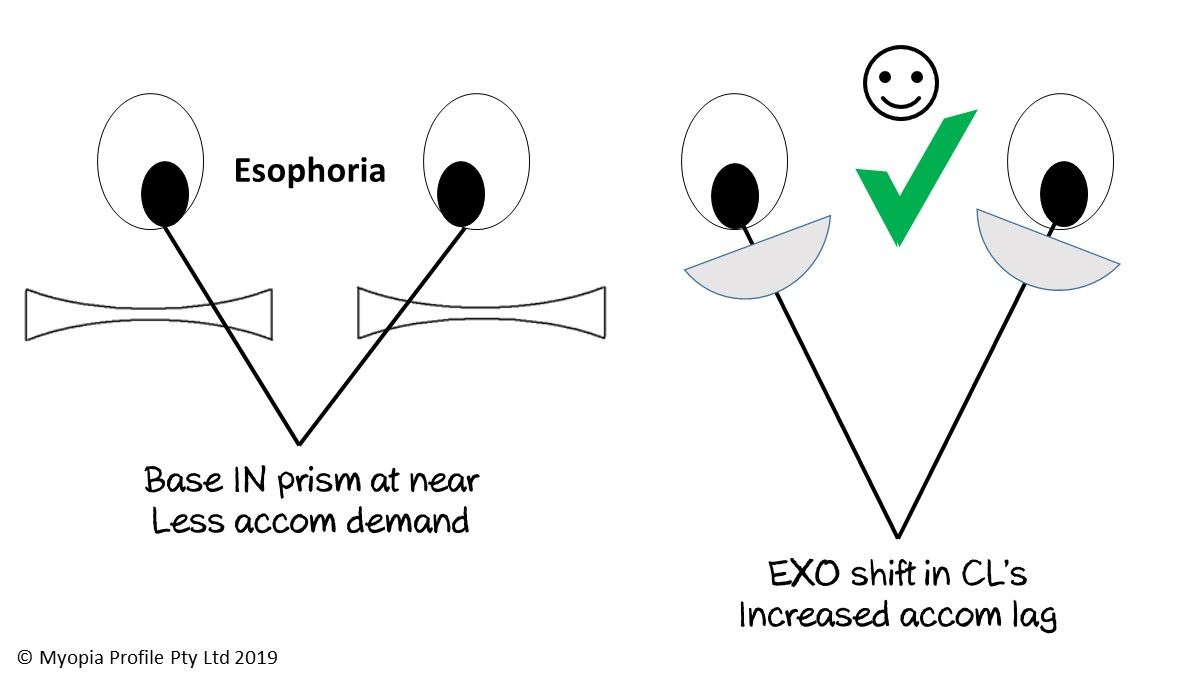
Binocular vision (BV) examination revealed a convergence excess esophoria of 4 prism dioptres (PD) at distance and 10PD at near. Additionally, Oliver showed a lead of accommodation, worse in his left eye (R +0.25 L -0.25), which was the likely source for his conflicting acuity and cycloplegic refraction results. Oliver had only ever worn spectacles and had recently been fit with his first pair of extended focus (progressive) lenses, but was interested in wearing contact lenses. In Oliver's case, contact lenses would serve three purposes better than spectacle correction: firstly to provide a better myopia control option,1 secondly to reduce the near esophoria by simply shifting from spectacles to contact lenses, and finally to see if the multifocal nature of either OK or MFSCLs could additionally help to improve his BV presentation.
In Oliver’s case, contact lenses would serve three purposes better than spectacle correction.
With corneal topography revealing corneae too flat for likely success with OK fitting, Oliver was fit with Coopervision Misight multizone daily disposable contact lenses in the powers R -6.00 L -5.50. After cycloplegia the immediate BV response to this optical change couldn't be measured, but two months later Oliver exhibited R 6/7.5+1 and L 6/9 contact lens acuity and his esophoria had improved to 2PD at distance and 7PD at near. He no longer exhibited a lead of accommodation (R&L +1.00) although he did show a L -0.50 refraction change, which better fit the acuity result this time than at the first examination. Oliver's L contact lens prescription was increased to avoid the potential for myopia progression from undercorrection2 and he was also prescribed divergence vision training to improve the still-evident convergence excess. In Oliver's case, it is not known how much his esophoria could additionally relax through wearing his multizone contact lenses, which feature concentric zones of the distance correction alternated with a +2.00 Add, as the research is still not clear on exactly how these lenses work in non-presbyopic eyes with active (and in this case, overactive) accommodation.
Do multifocal lenses and OK provide an 'add' at near? It's easy to understand why a MFSCL may provide an add for a non-presbyopic wearer, as the first MFSCL investigated for myopia control was a distance centred multifocal first developed for presbyopes.3 OK, in similarity, can be thought of as a distance centred multifocal, as the significant increase in positive spherical aberration generated through the corneal topographical change creates on-axis depth of focus. Positive spherical aberration occurs when peripheral light rays are focussed more myopically than the central light rays - in OK this owes to the mid-peripheral steepening generated. After just one week of OK wear in young adults, a measured shift in the correlation between corneal and total-eye aberrations indicates that an increased accommodative response occurs, which could effectively reduce accommodative lags.4
Want to learn more about binocular vision?
Check out my online course Binocular Vision Fundamentals, which starts with my two-system approach to BV assessment and diagnosis. Stepping through understanding of the accommodation and vergence systems, the course then covers clinical tests, diagnostic criteria, prescribing and management. Once this foundation is set, it moves onto clinical communication and the importance of BV in myopia management. Always with a laser sharp focus on the clinical applications.
Included are video examples of assessment techniques and chairside infographic summary downloads to reference in practice.
You can enroll on the first two modules for free, with the full course priced at US$140 if you decide to continue. Reduced course fees by 30% and 50% are available by application for practitioners residing in lower income countries - check out the course page for more information.
Meet the Authors:

About Kate Gifford
Dr Kate Gifford is an internationally renowned clinician-scientist optometrist and peer educator, and a Visiting Research Fellow at Queensland University of Technology, Brisbane, Australia. She holds a PhD in contact lens optics in myopia, four professional fellowships, over 100 peer reviewed and professional publications, and has presented more than 200 conference lectures. Kate is the Chair of the Clinical Management Guidelines Committee of the International Myopia Institute. In 2016 Kate co-founded Myopia Profile with Dr Paul Gifford; the world-leading educational platform on childhood myopia management. After 13 years of clinical practice ownership, Kate now works full time on Myopia Profile.
References
- Huang J, Wen D, Wang Q, McAlinden C, Flitcroft I, Chen H, Saw SM, Chen H, Bao F, Zhao Y, Hu L, Li X, Gao R, Lu W, Du Y, Jinag Z, Yu A, Lian H, Jiang Q, Yu Y, Qu J. Efficacy Comparison of 16 Interventions for Myopia Control in Children: A Network Meta-analysis. Ophthalmol. 2016;123:697-708. (link)
- Chung K, Mohidin N, O'Leary DJ. Undercorrection of myopia enhances rather than inhibits myopia progression. Vision Research. 2002;42:2555-2559. (link)
- Walline JJ, Greiner KL, McVey ME, Jones-Jordan LA. Multifocal contact lens myopia control. Optom Vis Sci. 2013;90:1207-1214. (link)
- Gifford P, Li M, Lu H, Miu J, Panjaya M, Swarbrick HA. Corneal versus ocular aberrations after overnight orthokeratology. Optom Vis Sci. 2013;90:439-447. (link)
- Tarrant J, Severson H, Wildsoet CF. Accommodation in emmetropic and myopic young adults wearing bifocal soft contact lenses. Ophthalmic Physiol Opt. 2008;28:62-72. (link)
- Aller TA, Liu M, Wildsoet CF. Myopia Control with Bifocal Contact Lenses: A Randomized Clinical Trial. Optom Vis Sci. 2016;93:344-352. (link)
- Gong CR, Troilo D, Richdale K. Accommodation and Phoria in Children Wearing Multifocal Contact Lenses. Optometry and Vision Science. 2017;94:353-360. (link)
- Kang P, Wildsoet CF. Acute and short-term changes in visual function with multifocal soft contact lens wear in young adults. Cont Lens Anterior Eye. 2016;39:133-140. (link)
- Gifford KL GP, Hendicott PL, Schmid KL. Near binocular visual function in young adult orthokeratology versus soft contact lens wearers. Cont Lens Anterior Eye. 2017;40:184-189. (link)
- Gifford KL GP, Hendicott PL, Schmid KL. Binocular visual function in orthokeratology contact lens wear for myopia. Invest Ophthalmol Vis Sci. 2017;58:ARVO E-Abstract 2683878. (link)
- Tarrant J, Liu Y, Wildsoet CF. Orthokeratology Can Decrease the Accommodative Lag in Myopes. Invest Ophthalmol Vis Sci. 2009;50:4294. (link)
- Anstice NS, Phillips JR. Effect of Dual-Focus Soft Contact Lens Wear on Axial Myopia Progression in Children. Ophthalmol. 2011;118:1152-1161. (link)
Enormous thanks to our visionary sponsors
Myopia Profile’s growth into a world leading platform has been made possible through the support of our visionary sponsors, who share our mission to improve children’s vision care worldwide. Click on their logos to learn about how these companies are innovating and developing resources with us to support you in managing your patients with myopia.