Clinical
The 'why' of myopia control
In this article:
Why Myopia Control? If we can slow down myopia progression this is a huge modifying factor for lifelong risk of visual impairment.
It is commonly understood that myopia prevalence is growing globally. By 2050, it is predicted that half of the world's population - five billion people - will be myopic, with nearly one billion at risk of myopia related ocular pathology.1 The late Brien Holden was a champion of ensuring myopia is placed on the world health agenda - high myopia is strongly linked to higher risk of cataract, retinal detachment and myopic maculopathy,2 and increasing rates of vision impairment and blindness due to the latter are already evident in Asian countries.3, 4 The World Health Organisation now recognises the public health issue of myopia, releasing a joint report with the Brien Holden Vision Institute in 2016.5
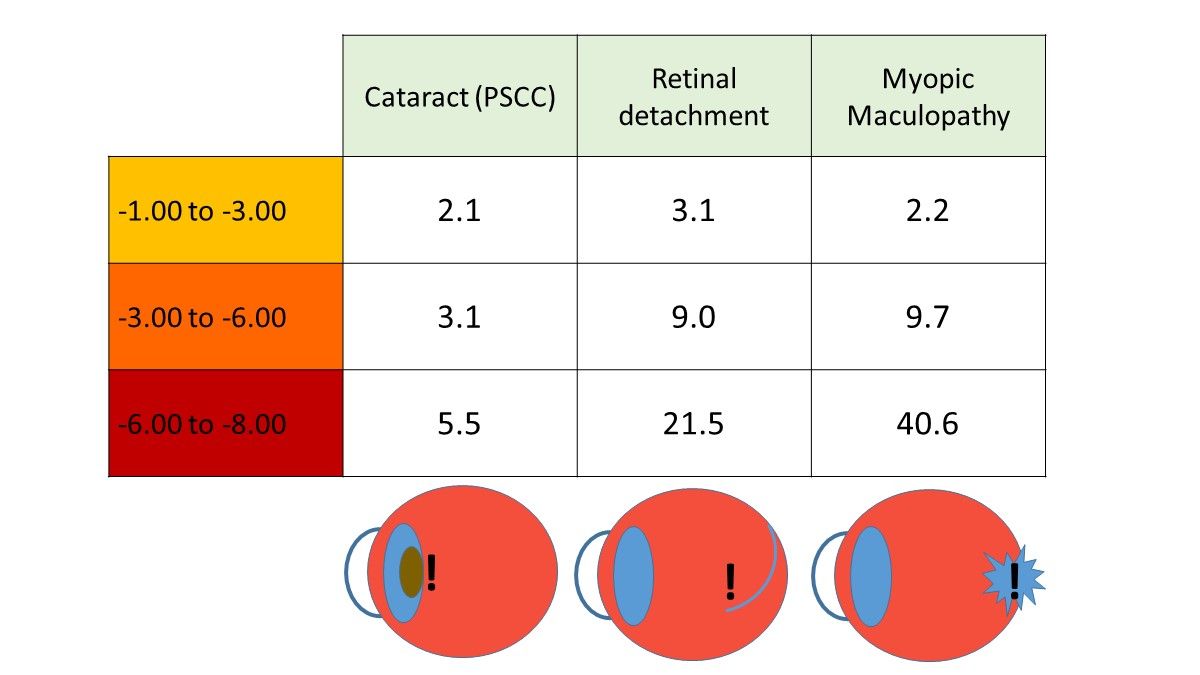
The myopia control imperative is understanding that even -1.00D of myopia carries an additional lifelong risk of posterior subcapsular cataract (PSCC), retinal detachment (RD) and myopic maculopathy (MM). A convincing case has been previously made by paediatric ophthalmologist Ian Flitcroft that the delineation of physiological and pathological myopia is not valid, as the term 'physiological' implies that there is a level of myopia which could be considered 'safe' in comparison to emmetropia.
Using odds ratios, which describe the increased risk of a condition over a reference of 1 (this being the risk of emmetropia), the image above summarises Flitcroft's data2 which shows that even 1D of myopia doubles the risk of MM and PSCC, and triples the risk of RD compared to the emmetrope. At 3D of myopia, the risk of PSCC triples, with the risk of RD and MM being nine times that of the emmetrope. Higher levels of myopia bring more eye-watering risks.
| Glaucoma | Cataract (PSCC) | Retinal Detachment | Myopic Maculopathy | |
| -1 to -3 | 2.3 | 2.1 | 3.1 | 2.2 |
| -3 to -5 | 3.3 | 3.1 | 9 | 9.7 |
| -5 to -7 | 3.3 | 5.5 | 21.5 | 40.6 |
| <-7 | - | - | 44.2 | 126.8 |
Axial length control
While dioptres of myopia are easily measurable and an indicator of risk, ultimately myopia control is about axial length control. Tideman and colleagues from the Netherlands evaluated the prevalence of lifelong visual impairment (6/12 or less) with increasing axial length, using data from over 10,000 Dutch people with an average age of 61 years - an axial length of 24-26mm was used as the referent.
Axial length of 26-28mm doubled the risk of visual impairment by age 60, while 28-30mm increased the risk by 11 times and an axial length of 30mm or more by 25 times. The prevalence of visual impairment by age 75 for the longest eyeballs (over 30mm) was 90%. Between 26-30mm axial length, the likelihood of being visually impaired by age 75 was around 25%, with the difference between shorter (26-28mm) and longer (28-30mm) eyes being the age of onset - the person with longer eyeballs is likely to suffer visual impairment for a longer duration of their life.6
Summarized in the table below, this is sobering data and provides the clear message to both patients and parents that controlling axial elongation also controls lifelong risk of visual impairment.
| Odds ratio of visual impairment by age 60 | Prevalence of visual impairment by age 75 | |
| 24-26mm | 1 (reference) | 4% |
| 26-28mm | 2 x risk | 25% |
| 28-30mm | 11 x risk | 27% |
| 30mm + | 25 x risk | 90% |
Myopia - like diabetes and glaucoma?
An analogy can be drawn to the association between diabetes and sugar intake. While suspected and observed historically, it was unclear whether multiple factors such as obesity, sedentary behaviour, consumption of other foods, ageing, urbanisation and income confounded the link between sugar intake and diabetes prevalence in overall populations. However recent data evaluating 175 countries, and controlling for each of this confounders, found a dose dependent relationship whereby every 150kcal per person per day increase in sugar availability was associated with an increased diabetes prevalence of 1.1%.7 Similarly, every part-millimetre increase in axial length in the myope brings an increased risk of pathology. Just as the optometrist will discuss the link between blood sugar level control and eye health; in the same way, myopia must be controlled to reduce risks to long-term eye health.
We can extend this analogy further to glaucoma - I'm sure it's safe to say that we're all good at explaining glaucoma, and its lifelong eye health risks, even though IOP isn't a clear cut diagnostic factor. In the same way, we can be just as good as explaining that more myopic dioptres, like IOP, increase eye health risk. Despite the fact that there's no guarantee that your -4.00 D patient will suffer maculopathy or retinal detachment in their lifetime, the risks are real, as they are for our patient with an IOP of 26mmHg, depending on their individual presentation. I'll go into more detail on this topic in the next lesson.
The key message is if that we can keep myopia below -3.00 and axial length below 26mm this is a huge modifying factor for lifelong risk of visual impairment.
Meet the Authors:

About Kate Gifford
Dr Kate Gifford is an internationally renowned clinician-scientist optometrist and peer educator, and a Visiting Research Fellow at Queensland University of Technology, Brisbane, Australia. She holds a PhD in contact lens optics in myopia, four professional fellowships, over 100 peer reviewed and professional publications, and has presented more than 200 conference lectures. Kate is the Chair of the Clinical Management Guidelines Committee of the International Myopia Institute. In 2016 Kate co-founded Myopia Profile with Dr Paul Gifford; the world-leading educational platform on childhood myopia management. After 13 years of clinical practice ownership, Kate now works full time on Myopia Profile.
References
- Holden BA, Jong M, Davis S et al. Nearly 1 billion myopes at risk of myopia-related sight-threatening conditions by 2050 - time to act now. Clin Exp Optom. 2015;98:491-3. (link)
- Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012;31:622-60. (link)
- Wu L, Sun X, Zhou X, Weng C. Causes and 3-year-incidence of blindness in Jing-An District, Shanghai, China 2001-2009. BMC Ophthalmol. 2011;11:10. (link)
- Iwase A, Araie M, Tomidokoro A et al. Prevalence and causes of low vision and blindness in a Japanese adult population: the Tajimi Study. Ophthalmology. 2006;113:1354-62. (link)
- World Health Organization. The impact of myopia and high myopia. 2016 Report.
- Tideman JW, Snabel MC, Tedja MS et al. Association of Axial Length With Risk of Uncorrectable Visual Impairment for Europeans With Myopia. JAMA Ophthalmol. 2016;134:1355-63.(link)
- Basu S, Yoffe P, Hills N, Lustig RH. The relationship of sugar to population-level diabetes prevalence: an econometric analysis of repeated cross-sectional data. PLoS One. 2013;8:e57873. (link)
Enormous thanks to our visionary sponsors
Myopia Profile’s growth into a world leading platform has been made possible through the support of our visionary sponsors, who share our mission to improve children’s vision care worldwide. Click on their logos to learn about how these companies are innovating and developing resources with us to support you in managing your patients with myopia.