Clinical
How to understand myopia risk factors
In this article:
Understand how the free-to-download, multi-language Managing Myopia Guidelines Infographic can be used as a chairside reference to identify risk factors for myopia development and progression, with the scientific basis of each described.
Identifying the pre-myope
Pre-myopia is defined by the International Myopia Institute1 as “a refractive state of an eye of ≤ 0.75 D and > 0.50 D in children where a combination of baseline refraction, age, and other quantifiable risk factors provide a sufficient likelihood of the future development of myopia to merit preventative interventions.”
There are four key risk factors for a child becoming myopic, or being a pre-myope. These can be used in assessing risk of myopia onset:
Family history - one myopic parent increases risk by three-fold, while two myopic parents doubles this risk again2
Visual environment - less than two hours per day spent outdoors increases risk,3 especially if combined with more than 3 hours a day spent on near work activities (outside of school time)4
Binocular vision - Children with higher accommodative convergence (AC/A) ratios, typically seen with esophoria, have an increased risk of myopia development within one year of over 20 times.5 Accommodative lag may also be a risk factor but there is conjecture.6 Intermittent exotropia has also been associated with onset of myopia.7
Current refraction - the most significant risk factor of this lot for future myopia is if a child exhibits less than +0.75D (cycloplegic) manifest hyperopia at age 6. See the highlight box below for more cut-offs based on age. This risk is independent of family history and visual environment. These thresholds for myopia risk in older children are +0.50D or less at ages 7 to 8, +0.25D or less at ages 9 to 10 and plano or less at age 11. These children are highly likely to be myopic by age 13.8
In addition to these, the fastest rate of refractive change in myopic children occurs in the year prior to onset,9 so the child who is less hyperopic than age normal should be closely monitored, especially if concurrent risk factors are evident.
The most significant risk factor for becoming myopic, independent of all other factors, is being less than +0.75D at age 6, +0.50D or less at ages 7 to 8, +0.25D or less at ages 9 to 10 and plano or less at age 11. These children are defined as pre-myopes and should be monitored more closely, with modifiable risk factors (visual environment and binocular vision) addressed where possible.
Identifying the child at risk of myopia progression
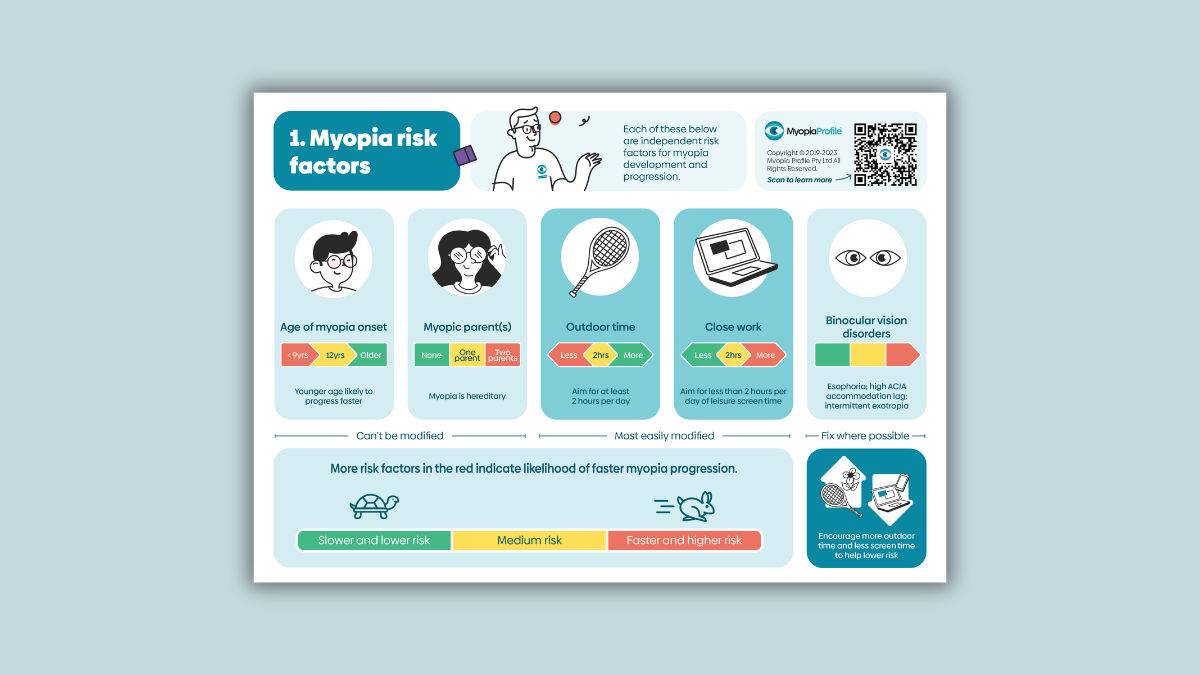
The principles of assessing a child’s risk for myopic progression is quite similar. The graphic above, from the free-to-download clinical resource Managing Myopia Guidelines Infographics, summarises the main aspects to consider when evaluating risks for myopia progression.
Age of myopia onset - the younger a child becomes myopic, the faster they will progress, with children 7 years of age progressing by at least 1D per year with this halving by age 11-12.10
Myopic parent(s) - children with two myopic parents have been shown to be the fastest progressors in single vision spectacle and atropine corrections, and children with one myopic parent progress less than the former but more than the child without such family history.11,12
Visual environment - near work at less than 20cm working distance and durations of longer than 45 minutes have been linked with more myopia progression. There is conflicting evidence regarding the efficacy of increased time spend outdoors in reducing myopia progression. It is still best practice to recommend outdoor time (minimum 2 hours per day) to improve a child’s visual environment.3,13
Binocular vision disorders – watch for esophoria, accommodative lag and intermittent exotropia. In myopia control studies of progressive addition spectacle lenses (PAL), children with esophoria in single vision spectacle control groups were found to progress more quickly, 14 and children with a larger baseline accommodative lag in the PAL groups showed statistically greater treatment effect.15 Children with lower baseline accommodative amplitude have shown a greater myopia control response to orthokeratology contact lens wear compared to normal accommodators.16 Finally, while the effect of controlling IXT on controlling myopia has not yet been studied, 50% of children with intermittent exotropia (IXT) are myopic by age 10 and 90% by age 20.7
In addition to the above, Asian ethnicity has been linked to faster myopia progression. 10,17
These risk factors can also be grouped in those that are modifiable and those that are not modifiable. Age of onset and parental history are unmodifiable and whilst useful to consider and communicate, no action is possible. Modifiable risk factors are the child’s visual environment, which includes time spent doing near work and outdoor time. Binocular vision disorders can also be modifiable, depending on the issues at hand.
The more risk factors the child has, the more likely he/she will progress. One may choose to initiate a more aggressive myopia management strategy if the risk factors suggest fast progression.
Essentially, any myopic child is a progressor until proven otherwise! The institution of a myopia control strategy as early as possible is evidence based practice, especially before age 10 when progression is fastest. The Myopia Profile Managing Myopia Guidelines Infographic and patient brochure (free to download and available in numerous language translations) is designed to help you explain risk and the steps a parent or carer can take to modify risk factors, where applicable.
The Managing Myopia Guidelines Infographics
Myopia Profile’s popular and entirely free Managing Myopia Guidelines Infographics are designed to support clinical communication and decision making in myopia management. These engaging infographics are available to download and print in several formats and numerous language translations.
There are two four-panel infographics which can be printed in large format as poster (ANSI-C or A2), or scaled down to US Letter or A4 to be used as a handheld infographic for in-room discussions and reference.
The mostly blue infographic is a chairside reference guide for eye care professionals that guides you through: (1) Myopia risk factors, (2) What to prescribe, (3) Follow-up schedules and (4) Gauging success
The multi-colored infographic is designed to help you communicate with parents and patients on the following topics: (1) Visual environment advice, (2) What are my options? (3) Kids can wear contact lenses and (4) Why myopia management is essential.
The Infographics can also be printed as individual panels (US Letter and A4 sizes) to use each page on its own if you prefer. As above, there are four which are parent- and patient-facing (multi-coloured) and four which are your chairside reference (mostly blue coloured). The image below shows various print formats, with all panels collated (at back) and single pages (foreground).
Freshly updated in late 2023 and built from the ground up from continued feedback with eye care practitioners and industry advisers, these Managing Myopia Guidelines Infographics are designed to be used by eye care professionals, in discussion with patients and their carers, and as a clinical reference.
For an overview of how to use the Infographics in practice, read our article Using the Managing Myopia Guidelines Infographics
For guidance on the guided clinical communication process provided the Infographics, read our article Keys to Communication in Myopia Management.
Once you have used the Infographics to explain myopia to patients and their parents or carers in your exam room, these messages can be further enhanced by providing the take-home, free-to-download Managing Myopia patient brochure.
Meet the Authors:

About Kate Gifford
Dr Kate Gifford is an internationally renowned clinician-scientist optometrist and peer educator, and a Visiting Research Fellow at Queensland University of Technology, Brisbane, Australia. She holds a PhD in contact lens optics in myopia, four professional fellowships, over 100 peer reviewed and professional publications, and has presented almost 300 conference lectures around the world. Kate is the Chair of the Clinical Management Guidelines Committee of the International Myopia Institute. In 2016 Kate co-founded Myopia Profile with Dr Paul Gifford; the world-leading educational platform on childhood myopia management. After 13 years of clinical practice ownership, Kate now works full time on Myopia Profile.

About Kimberley Ngu
Kimberley is a clinical optometrist from Perth, Australia, with experience in patient education programs, having practiced in both Australia and Singapore.
Read Kimberley's work in many of the case studies published on MyopiaProfile.com. Kimberley also manages our Myopia Profile and My Kids Vision Instagram and My Kids Vision Facebook platforms.
References
- Flitcroft DI, He M, Jonas JB, Jong M, Naidoo K, Ohno-Matsui K, Rahi J, Resnikoff S, Vitale S, Yannuzzi L. IMI - Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Invest Ophthalmol Vis Sci. 2019 Feb 28;60(3):M20-M30. (link)
- Jones LA, Sinnott LT, Mutti DO, Mitchell GL, Moeschberger ML, Zadnik K. Parental History of Myopia, Sports and Outdoor Activities, and Future Myopia. Invest Ophthalmol Vis Sci. 2007;48:3524-3532. (link)
- Xiong S, Sankaridurg P, Naduvilath T, Zang J, Zou H, Zhu J, Lv M, He X, Xu X. Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review. Acta Ophthalmol. 2017 Sep;95(6):551-566. (link)
- Rose KA, Morgan IG, Ip J, Kifley A, Huynh S, Smith W, Mitchell P. Outdoor Activity Reduces the Prevalence of Myopia in Children. Ophthalmol. 2008;115:1279-1285. (link)
- Mutti DO, Jones LA, Moeschberger ML, Zadnik K. AC/A Ratio, Age, and Refractive Error in Children. Invest Ophthalmol Vis Sci. 2000;41:2469-2478. (link)
- Mutti DO, Mitchell GL, Hayes JR, Jones LA, Moeschberger ML, Cotter SA, Kleinstein RN, Manny RE, Twelker JD, Zadnik K, the CLEERE Study Group. Accommodative Lag before and after the Onset of Myopia. Invest Ophthalmol Vis Sci. 2006;47:837-846. (link)
- Ekdawi NS, Nusz KJ, Diehl NN, Mohney BG. The development of myopia among children with intermittent exotropia. Am J Ophthalmol. 2010;149(3):503-507. (link)
- Zadnik K, Sinnott LT, Cotter SA, Jones-Jordan LA, Kleinstein RN, Manny RE, Twelker JD, Mutti DO, Collaborative Longitudinal Evaluation of E, Refractive Error Study G. Prediction of Juvenile-Onset Myopia. JAMA Ophthalmol. 2015;133:683-689. (link)
- Mutti DO, Hayes JR, Mitchell GL, Jones LA, Moeschberger ML, Cotter SA, Kleinstein RN, Manny RE, Twelker JD, Zadnik K. Refractive error, axial length, and relative peripheral refractive error before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2007;48:2510-2519. (link)
- Donovan L, Sankaridurg P, Ho A, Naduvilath T, Smith ELI, Holden BA. Myopia progression rates in urban children wearing single-vision spectacles. Optom Vis Sci. 2012;89:27-32. (link)
- Kurtz D, Hyman L, Gwiazda JE, Manny R, Dong LM, Wang Y, Scheiman M. Role of parental myopia in the progression of myopia and its interaction with treatment in COMET children. Invest Ophthalmol Vis Sci. 2007;48(2):562-570. (link)
- Loh KL, Lu Q, Tan D, Chia A. Risk factors for progressive myopia in the atropine therapy for myopia study. Am J Ophthalmol. 2015;159:945-949. (link)
- Huang PC, Hsiao YC, Tsai CY, Tsai DC, Chen CW, Hsu CC, Huang SC, Lin MH, Liou YM. Protective behaviours of near work and time outdoors in myopia prevalence and progression in myopic children: a 2-year prospective population study. Br J Ophthalmol. 2020 Jul;104(7):956-961. (link)
- Yang Z, Lan W, Ge J, Liu W, Chen X, Chen L, Yu M. The effectiveness of progressive addition lenses on the progression of myopia in Chinese children. Ophthal Physiol Opt. 2009;29:41-48. (link)
- Gwiazda J, Hyman L, Hussein M, Everett D, Norton TT, Kurtz D, Leske MC, Manny R, Marsh-Tootle W, Scheiman M. A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Invest Ophthalmol Vis Sci. 2003;44:1492-1500. (link)
- Zhu M, Feng H, Zhu J, Qu X. The impact of amplitude of accommodation on controlling the development of myopia in orthokeratology. Chinese J Ophthalmol. 2014;50:14-19. (link)
- Hyman L, Gwiazda J, Hussein M, Norton TT, Wang Y, Marsh-Tootle W, Everett D. Relationship of age, sex, and ethnicity with myopia progression and axial elongation in the correction of myopia evaluation trial. Arch Ophthalmol. 2005;123(7):977-987. (link)
Enormous thanks to our visionary sponsors
Myopia Profile’s growth into a world leading platform has been made possible through the support of our visionary sponsors, who share our mission to improve children’s vision care worldwide. Click on their logos to learn about how these companies are innovating and developing resources with us to support you in managing your patients with myopia.